Opioid patches – back to basics
The two opioids available for delivery via a transdermal patch in the UK are fentanyl and buprenorphine. Fentanyl products are licensed for severe and chronic pain that requires long-term opioids or that does not respond to non-opioids.
Buprenorphine is available in two sets of products – the stronger patches have a similar license to fentanyl while the lower strengths are indicated for non-malignant pain when an opioid is necessary (they are used for cancer pain in some cases, where patients only require low opioid doses).
Patches are only suitable for stable pain as they take up to 24 hours to reach steady state, so they should only be used for people whose pain is not rapidly increasing.
All fentanyl patches are effective for 72 hours once applied. The stronger buprenorphine patches remain effective for 96 hours (apart from one brand) but the weaker ones only need to be replaced once a week and this can be confusing for prescribers who are unfamiliar with these medicines.
We should advise patients to find the best way to remind themselves of the day they must change their patch – some might want to mark it on a calendar while others prefer to set a reminder on their smart phone.
Positive points
- Convenient method of delivery.
- Enables people to think a bit less about their medication and live their life.
- They can be applied on various parts of the body, the site should be rotated to minimise the risk of irritation after repeated applications to one spot.
- Useful for people who may have problems remembering to take medicines.
- Useful for people:
– with cognitive impairment
– who struggle with oral medicines or have nausea and vomiting or e.g. oral cancers. - Appropriate for people with renal insufficiency.
- The wide variation in strengths available makes it possible to tailor the dose appropriately.
Cautions
- Once applied, patches take several hours to reach therapeutic levels so other analgesia should be available.
- If the dose selected is too high for the patient and they become toxic, drowsy, even unrousable, just taking the patch off won’t be enough to assure their safety as it takes up to 24 hours for levels to decrease. If the patient has become sufficiently drowsy to require opioid reversal, ensure expert advice is sought.
- Patches can be especially dangerous in this respect for initiation in frail elderly patients on their own at home – they must be monitored.
- If a patient is being switched from oral opioids to a patch the prescriber should use the guide on the SPC or the local guidelines for this. The fentanyl patches cover a wide range of possible doses so the lower doses should be used initially, e.g. fentanyl 25mcg patch is equivalent to between 90 and 134mg total daily morphine, which makes it challenging to safely convert.
- Heat increases absorption – avoid hot showers/baths and caution in extreme hot weather, like we have experienced recently. We need to alert patients and carers about this without alarming them – remind them to be aware of promptly reporting toxic effects.
- People should be given PRN opioids alongside the patch – this can be morphine if they are not being used because of renal insufficiency. Check in conversion tables to make sure the PRN dose is commensurate.
- Fentanyl immediate release products, e.g. Abstral, are not intended for use for PRN support in the same way as we use morphine and oxycodone in one sixth of the daily dose.
- GPs can sometimes be a bit more relaxed about prescribing patches. Remember that fentanyl is between 100 and 150 times as potent as morphine so it must be treated with respect.
- All but one brand of patches are now ‘matrix’ patches, where the product is embedded in a plastic film or textile. Occasionally it used to be recommended to cut patches, but now with a range of strengths available, this should not be necessary. It is off licence but not dangerous, however there are still a few products which are ‘gel-filled’ patches (the older formulation) which must never be cut.
- Some people have problems with patches that won’t stick because of sweating or oily skin – try a different brand.
- Some people have an allergic reaction to the patch, but this is invariably due to the adhesive and not the drug – try a different brand. (One unlicensed and imaginative way to reduce irritation is to spray the area with a steroid using an inhaler e.g. beclometasone).
Ensure people read the instructions – when applying a patch, hold it down for 20 seconds to improve adhesion.
They can be disposed of in general waste – on removal, fold the patch in on itself. Patches still contain a lot of fentanyl/buprenorphine once removed so still should be disposed of carefully.
Product selection
There are many products available, although each product with the same strength is therapeutically equivalent. We advise you order using the trade name and aim to keep to one brand if possible – to make stock-keeping simpler and provide a familiar product to your patients. Although wards must order complete packs for stock, pharmacies will supply the quantity specified to complete an individual prescription.
As with many medicines, prices change periodically and although there are not huge differences between the brands, it can make a difference to your drugs budget when you use quantities. Ashtons pharmacists can provide guidance on the most cost-effective choices when we visit and attend medicines management meetings.
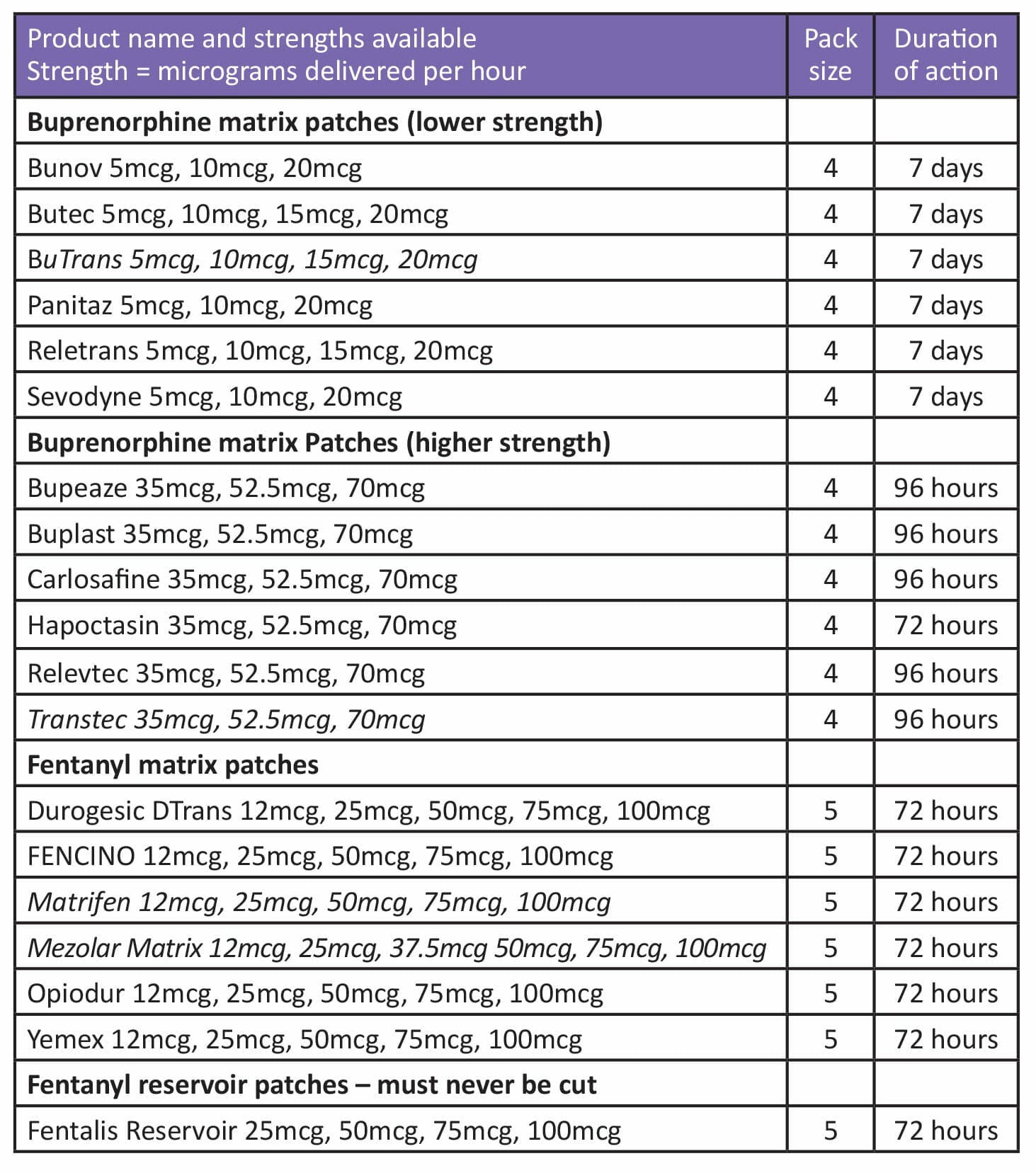
The table below shows the main products available but only includes those where there is a Summary of Product Characteristics available on the Electronic Medicines Compendium. Note one of the buprenorphine patches needs changing every 72 hours which makes it slightly less convenient for patients and as more are required, slightly more expensive. All but one of these products is a matrix patch where the drug is evenly distributed across the surface. One remains a ‘reservoir’ patch where the active ingredient is in a gel released via a membrane. Cutting patches is inadvisable at any time but on no account must a reservoir patch be cut.
Recent Insights



