Serotonin toxicity – are we missing it?
It is generally accepted that the management of symptoms in palliative care must involve appropriate polypharmacy. We are comfortable with using more than one medicine to help with one symptom provided the mechanisms of action are different and complementary – for example morphine plus gabapentin for pain with neuropathic characteristics. At the same time, we need also to be aware of the propensity for drugs with different mechanisms to cause the same adverse effects.
Serotonin or 5-hydroxytryptamine (5HT) is a naturally occurring neurotransmitter with at least 12 potential receptor sub-types associated with complex and multiple functions. We may think of it more in relation to the modulation of cognition and mood but only about 1-2% of total serotonin circulates within the central nervous system (CNS). It is mainly secreted from neuroendocrine cells in the gastro-intestinal tract and about 10% is transported on platelets in the blood where it acts mainly as a vasoconstrictor and regulator of haemostasis(1).
It is probably mostly associated therapeutically with depression as while there is certainly a connection between serotonin and depression, the direction of this relationship is unclear. It is not known whether low serotonin causes depression, or whether depression causes low serotonin. It is metabolised in the liver by monoamine oxidase hence the use of drugs that inhibit its breakdown – monoamine oxidise (MAOIs) – as antidepressants. These are rarely used now, but more recent SSRIs (specific serotonin re-uptake inhibitors) achieve the same goal of increasing circulating serotonin with the aim of improving mood. However, if levels of serotonin become too elevated and synaptic concentration in the CNS is raised, the effects can lead to toxicity which may be fatal if untreated.
Symptoms of serotonin toxicity
There are no tests for what used to be called ‘serotonin syndrome’ so the clinical picture is constructed from the symptoms which fall into three categories:
- Autonomic – sweating, fever, tachycardia, hypertension, tachypnoea, sialorrhea, diarrhoea
- Neuromuscular – tremor, hyperreflexia, myoclonus, clonus
- Mental status – agitation, altered consciousness, hypomania, delirium
All symptoms may not be present and they can develop as rapidly as after one or two doses or gradually with less severe symptoms before building up to full toxicity. A case history(4) describes a patient taking mirtazapine and paroxetine for depression who developed serotonin toxicity presenting as hyperactive delirium, rigidity and hyperreflexia after 48 hours treatment with tramadol for pain from a recently diagnosed metastases from her pancreatic cancer. Another recent case reports onset after a single low dose of methadone being used as an adjunct to oxycodone and duloxetine(5). The patient had chills, tremors and was perspiring but recovered as the effects of the methadone dose wore off. We also discussed a recent case with a colleague (see case study below).
Case Study
Celia is a 56-year-old woman with an advanced neuroendocrine tumour. She has had chronic severe pain for the last year and unfortunately had become dependent on rapid release Fentanyl tablets (800 mcg up to 7 times a day). She was admitted to a palliative inpatient unit to explore whether alternative opioid regimes may help her pain. She was lucid and co-operative on admission. Soon after admission her Mirtazapine was increased from 15 mg to 30 mg as her mood was low.
She was already on 3 mg of Methadone that had been started in the community in the hope of reducing her Fentanyl use. As an inpatient it was felt that as Fentanyl had always helped her pain, maybe an Alfentanil infusion may be helpful. This was started in a relatively low dose over 24 hours. The next day the patient became tachycardic, much more confused, very breathless and agitated. She was hyperreflexive and sweating and not obviously opioid toxic.
The possibility of serotonin toxicity was considered as there was no other obvious cause for the sudden onset of her distressing symptoms.
It was established at that stage that she was on several medications that raised serotonin levels on a background of a tumour that might already have raised baseline serotonin.
The background of Methadone, the increase of Mirtazapine and the addition of a Fentanyl infusion clearly triggered a serotonin crisis.
The patient was hydrated and sedated with large doses of benzodiazepines and antipsychotic medication. Methadone was stopped, Mirtazapine was stopped and the Alfentanil infusion was switched a low dose Diamorphine infusion. Over the next few days her agitation reduced and she left the inpatient unit 10 days later in a calm, non- confused state.
She was maintained on a small dose of modified release Morphine and a more limited supply of rapid release Fentanyl tablets (600mcg, up to 5 x daily).
Three weeks after discharge, her condition was still stable at home but there are multiple warnings to avoid any medication that could increase her serotonin levels.
Treatment
If the symptoms are severe with the patient showing haemodynamic instability, temperature above 38.5°C, rigidity, advice should be sought from a critical care colleague with a view to transfer to acute care. If less severe, all potentially serotonergic medicines should be stopped and the symptoms will generally resolve within 24 hours. If treatment is required, the mainstay is midazolam at a dose of 5-10mg SC p.r.n. which will help manage agitation, myoclonus and seizures. The use of 5HT antagonists is suggested in the PCF7 – such as chlorpromazine 50-100mg IM cyproheptadine 12mg PO stat and then repeated at reduced doses. The perceived rarity of serotonin toxicity means that these rescue medications are rarely, if ever seen in hospices but it may be a discussion to have if we start to look out for this condition with more acuity.
Drug which increase serotonin levels
Although we know about the mechanisms of the antidepressants, we need to be aware of other drugs that can increase circulating serotonin levels which may be less obvious. These are listed in Table 1, below(2,3).
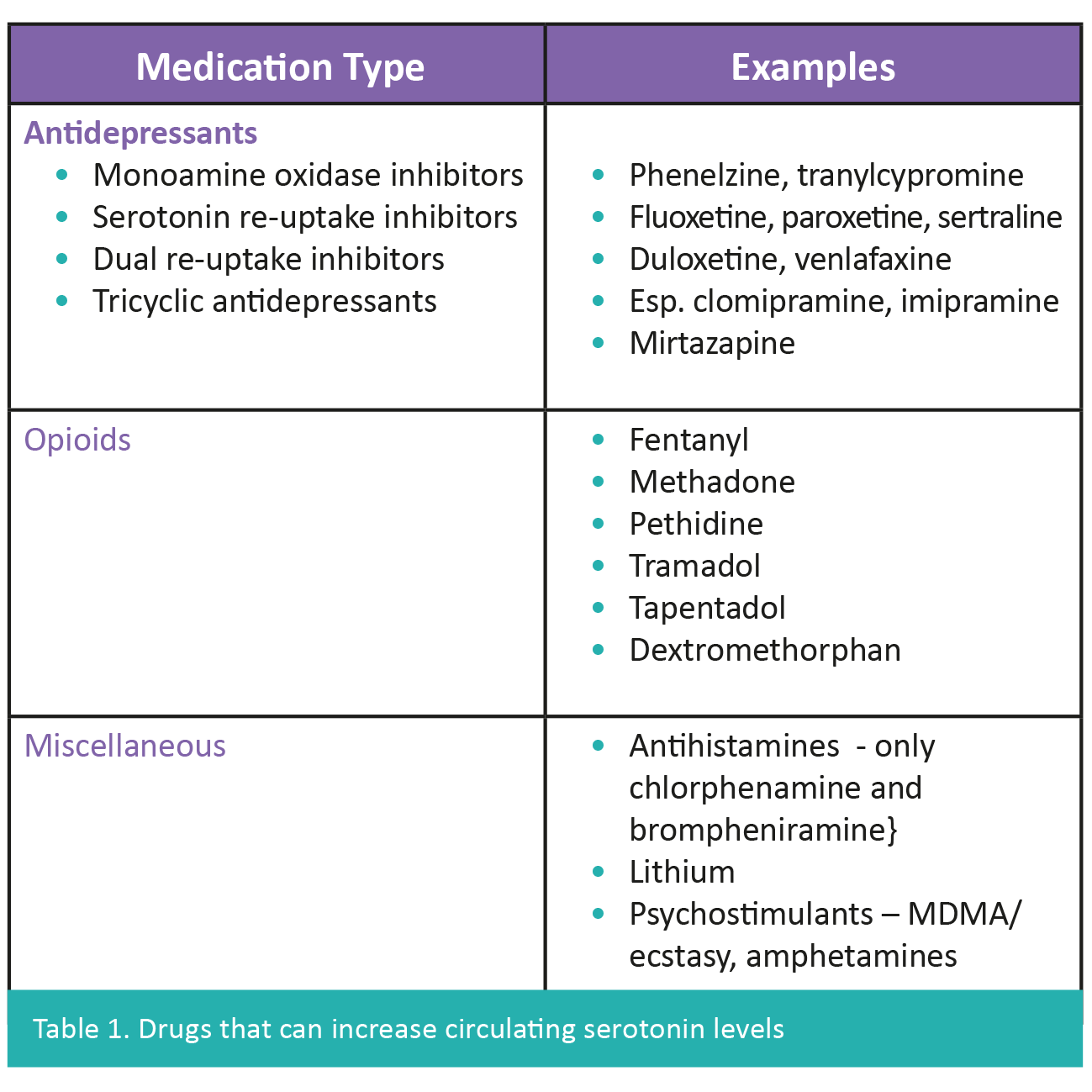
As well as the drugs listed to the right, we need to be aware of other drugs which use or inhibit the same liver enzymes for breakdown which can also increase circulating levels e.g. ciprofloxacin and cimetidine both induce the cytochromes that metabolise the tricyclic antidepressants (CYP1A2) and fentanyl (CYP3A4).
As often seems the case in palliative care, many of these symptoms if seen alone or when relatively mild would not necessarily be associated with serotonin and could be mis-interpreted as due to other causes
Summary
As often seems the case in palliative care, many of these symptoms if seen alone or when relatively mild would not necessarily be associated with serotonin and could be mis-interpreted as due to other causes e.g. the autonomic symptoms could suggest sepsis. A review article from Canada suggests that delirium is present in up to 42% of palliative care patients and that a proportion of these cases could be due to iatrogenic effects of drugs(6). It is thought that most cases of serotonin toxicity are provoked by therapeutic doses of a combination of two or more serotonergic drugs(7).
We are highlighting this topic as we feel it is important to remind clinicians to be aware of serotonin toxicity as a possible cause of unexpected symptoms which mimic e.g. terminal agitation. We also want to draw additional attention to some of the regularly used drugs which may not immediately make us think about serotonin – especially fentanyl and particularly when the background dose is already high.
References
Recent Insights



